
Certified Community Behavioral Health Clinics (CCBHCs) bring comprehensive mental health, substance use, and crisis services to millions of individuals in the United States. From 66 clinics in 8 states at program launch in 2017 to today’s more than 500 clinics in 46 states, Washington DC, and Puerto Rico, the proliferation of CCBHCs suggests the appeal of this health care model. Data substantiates its effectiveness, with significant decreases in mental health hospitalizations, homelessness, and time spent in jail noted among people who receive care at CCBHCs.
Expanding and strengthening services to respond to the needs of people with mental health conditions or substance use disorders is critical to healthy communities, and this is nowhere truer than among individuals in contact with the criminal justice system. CCBHCs are rising to the challenge.
The CCBHC Model
Congress established the CCBHC model as a demonstration program in the 2014 passage of the Protecting Access to Medicare Act. Section 223 of that Act called for criteria for participation in the demonstration program, as well as a payment structure applicable to medical assistance for mental health services. The Substance Abuse and Mental Health Services Administration (SAMHSA) issued the required criteria in 2015 and updated them in 2023.
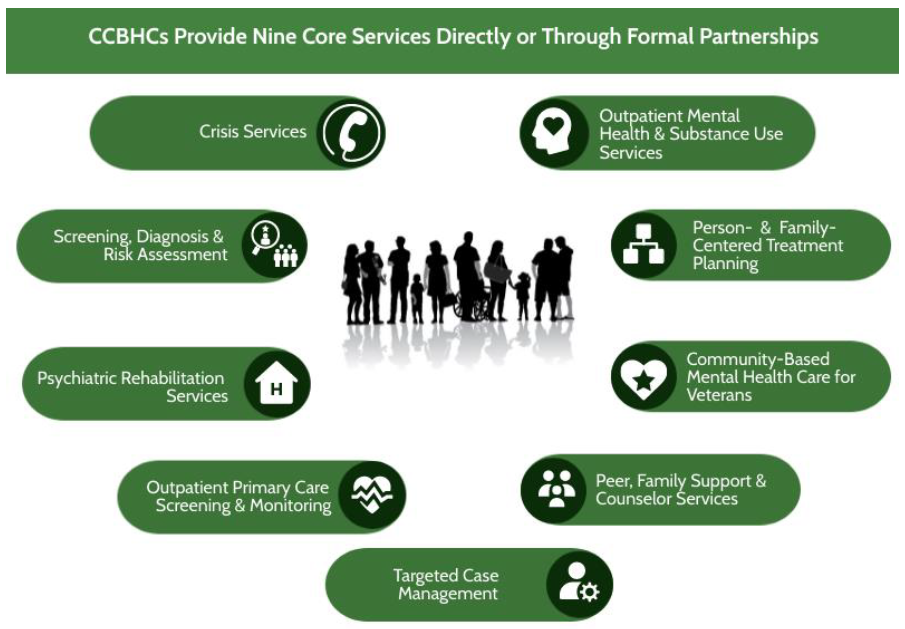
Figure 1. Source: SAMHSA. Certified Community Behavioral Health Center (CCBHC) Certification Criteria. Published February 2023. Accessed March 14, 2025, at https://www.samhsa.gov/sites/default/files/ccbhc-criteria-2023.pdf.
“The CCBHC criteria provide standards on staffing, availability and accessibility of services, care coordination, scope of services, quality and other reporting, and governance specifically for mental health and substance use,” said Brett Beckerson, senior director for public policy and advocacy at the National Council for Mental Wellbeing. “Essentially, they set the stage for one-stop shops for all behavioral health needs so that anyone, regardless of where they live or their ability to pay, can access services in an easy and expedited way.”
CCBHCs provide nine types of services (Figure 1), which must be coordinated and integrated across the health care system and other social service sectors to meet the recipients’ full range of needs. Funding for the activities of CCBHCs in the Section 223 Demonstration Program1 comes through Medicaid’s prospective payment system, created in response to the original statute.
A community needs assessment, required of all demonstration program participants, informs CCBHC’s staffing, services, locations, service hours, and evidence-based practices.
CCBHCs and the Criminal Justice System
The community needs assessment also identifies individuals with unmet care needs within the service area so that outreach, engagement, and retention activities can be appropriately planned and carried out.
“CCBHCs should explore how to work with the criminal justice system to meet everyone’s needs, particularly when a service area includes jails or prisons,” Beckerson said. “The federal legislation requires core coordination, but states are free to define the CCBHC-justice partnership, whether that be with specialty courts, jails, probation and parole, or throughout the entire range of the Sequential Intercept Model (SIM).”
In fact, 98 percent of CCBHCs actively partner with criminal justice agencies in a wide range of activities. The most common collaborative activities follow:
- Providing services or taking referrals in partnership with courts (including specialty courts)
- Increasing outreach and/or access to individuals who have criminal justice system involvement or are at risk of becoming involved
- Training law enforcement or corrections officers in Mental Health First Aid, Crisis Intervention Team principles, or other mental health/substance use disorder awareness training
- Offering postcrisis wraparound services to facilitate linkage and follow-up system.
CCBHCs Supported by a SIM Mapping in Missouri
Missouri took its community needs assessment a step further by conducting SIM mapping workshops in each of its 114 counties, plus the city of Saint Louis. This valuable step yielded an in-depth understanding of what resources and services were already in place, what was working, what was missing, and what could be improved.
“The SIM Mapping Workshops really clarified the opportunities CCBHCs have to strengthen the safety net for individuals who are at risk of entering, or already involved with, the criminal justice system,” reflected KC Rafferty, director of community engagement at the Missouri Behavioral Health Council (MBHC). “But perhaps more importantly, the workshops brought together stakeholders—behavioral health, law enforcement, prosecutors, probation/parole, and others—to collaborate and communicate in new ways.”
The Statewide SIM Collaboration Project was funded through a grant from the Missouri Foundation for Health and carried out as a unique partnership between MBHC, the Missouri Department of Mental Health, the Office of State Courts Administrator, the National Center for State Courts, and Policy Research Associates. Rafferty wholeheartedly believes that each partner is committed to finding better ways to divert individuals from the criminal justice system and to connect those who are in the justice system with behavioral health services as needed.
The SIM Mapping Workshops heightened awareness about resources available for people in crisis. Tapping behavioral health crisis centers or connecting with community behavioral health liaisons, for example, make it less likely that 911, law enforcement, or the justice system will be necessary.
Another outcome of the SIM mapping workshops was the pilot of jail reentry navigators, who provide case management services for individuals as soon as they are booked into jail (Intercept 2 of the SIM). CCBHC staff, located at the jail, often fill this dedicated role, which greatly assists jails struggling with funding and staffing constraints, such as those in rural areas. The navigators facilitate immediate connections to treatment, housing, transportation, and other support available upon release, and provide training to jail staff on responding to someone in a behavioral health crisis or some other type of emotional distress.
“Missouri started with the demonstration project in 2017, and we now have CCBHC coverage statewide,” said Rafferty. “Amazing things have happened at the local level simply through collaboration and leveraging what’s in place, but we also have the innovation and adaptability that the CCBHC model provides to really meet the needs of our community and to pursue additional initiatives.”
One CCBHC Serving Intercepts 0-5 across Oklahoma
GRAND Mental Health, which serves 13 counties in northern Oklahoma, also embraces the transformative opportunities offered by the CCBHC model for individuals at risk of or in contact with the criminal justice system. Oklahoma was one of the eight original states that participated in the demonstration program. The effort was timely: mental health crises among community members were surging beyond the capacity of law enforcement and emergency departments to respond, resulting in unmet needs, overuse of jail detention, and inefficient use of resources.
Supporting Individuals Before Crisis Escalates
Changes in staffing, technology, and other resources made possible through the demonstration program expedited implementation of a response system for individuals needing mental health care but not warranting inpatient hospitalization. Referred to as Grand Response Access Network on Demand, this system involves trained clinicians at Urgent Recovery Centers who respond to crisis calls, some of which come through a 24/7 crisis line. Calls also originate from specially programmed tablet computers that feature a crisis button for instant access to a therapist, as well as functionality for clinicians to conduct therapy sessions virtually. The tablets are distributed to patients, first responders, and other service providers.
“The tablets were a real game-changer for us as a strategy at Intercept 0,” observed Alicia Beard, operational director at GRAND Mental Health. “For many years, GRAND operated in primarily rural areas, where lack of transportation hindered care. The tablets broke down that barrier, allowing us to help individuals before a crisis escalates.” Evaluation results corroborate this: More adults received services (an increase of 164 percent), but far fewer required inpatient hospitalization (a decrease of 93 percent). Moreover, law enforcement shaved off 576 workdays spent transporting individuals in crisis, saving $718,000.
De-escalation also occurs at Intercept 1, where GRAND partners with law enforcement for safer outcomes. For example, Crisis Intervention Response Teams made up of mental health professionals and law enforcement officers respond to mental health-related calls for appropriate intervention. GRAND also ensures that all law enforcement officers receive Crisis Intervention Team training, equipping them to handle mental health situations safely and effectively.
Connecting Individuals to the Right Treatment
CCBHC staff focus on early treatment and appropriate services at Intercepts 2 and 3. In collaboration with Justice Link, which is a community-based resource hub, GRAND provides mental health and substance use services to individuals after arrest and before trial, thereby helping expedite case resolutions and reduce recidivism.
In multiple counties, GRAND provides free screening for substance use and mental health risk factors that help courts determine the most effective and least restrictive option at sentencing for individuals facing non-violent charges. Screening results often lead to specialty courts or community sentencing. GRAND holds contracts to provide services for drug court and mental health court, as well as family treatment court.
Preparing Individuals for Community Reentry
Dedicated to making a difference at every intercept, GRAND recently launched Release to Recovery in two counties. This program embeds GRAND staff within jails to conduct screenings and connect individuals to outpatient services, housing, and employment programs upon release.
Similar connections are forged for individuals in state prisons who have stimulant or opioid diagnoses. In partnership with the Department of Corrections, GRAND staff members call patients and their case managers prior to release to discuss and arrange connection to outpatient services for continued care and treatment immediately upon exit from prison. It is critical that medication-assisted treatment (MAT) not lapse. To that end, 80 percent of CCBHCs country-wide offer one or more forms of medications for opioid use disorder.
Regarding Intercept 5, GRAND maintains strong relationships with probation and parole officers to ensure ongoing access to mental health and substance use services for individuals under community-based criminal justice supervision. GRAND also provides services documentation attesting to individuals’ fulfillment of court requirements.
Looking Forward
The CCBHC model continues to evolve as new states and districts receive CCBHC Medicaid Demonstration Program planning grants, and long-established clinics, such as GRAND, continue to enhance services. Beckerson envisions a future where every clinic is working at every intercept to meet the needs of an entire community. Documenting CCBHC achievements can drive sustainability efforts by demonstrating how states are leveraging local resources. Rafferty concluded, “The CCBHC model has provided hope in Missouri by reinforcing the great things we do but also empowering us to go after more.”
For more information
- Missouri Behavioral Health Council’s KC Rafferty at krafferty@mobhc.org
- GRAND Mental Health’s Alicia Beard at abeard@GrandMH.com