
The high prevalence of mental and substance use disorders among individuals in contact with the criminal justice system is widely acknowledged, but how these issues intersect with what are commonly referred to as intellectual and developmental disabilities (IDD) is far less recognized. To comply with protections afforded under Section 504 of the Rehabilitation Act of 1973 and Title II of the Americans with Disabilities Act, first responders, court staff, forensic evaluators, and correctional personnel should aim to have a working knowledge of neurodevelopmental disorders (NDD).
NDD
“Neurodevelopmental disorders” are a group of conditions marked by functional impairment in personal, social, academic, and occupational domains. These disorders manifest before adulthood. IDD and autism spectrum disorder (ASD) are among the several types of NDD that are more prevalent among individuals in forensic settings than in the general population.
IDD
Figure 1
As many as 40 percent of individuals in the criminal justice system have been identified as having IDD, but this estimated prevalence varies considerably depending on research parameters and definitions. Individuals with IDD have challenges in both intellectual functioning (figure 1) and adaptive functioning, the latter being the ability to meet developmental and sociocultural standards for communication, social participation, and/or independent living. The severity of the disability can range from mild to profound; individuals in the criminal justice system with IDD are more likely to be at the mild range of the spectrum.
ASD
In some population studies, 10 percent of individuals in prison between ages 18 and 25 meet criteria for a diagnosis of ASD, a neurodevelopmental disorder characterized by two symptom categories:
| Deficits in social communication | Restricted interests and repetitive behaviors |
|---|---|
|
|
| Deficits in social communication | Restricted interests and repetitive behaviors |
|---|---|
|
|
Co-morbidities
Overlapping NDD is common. For example, approximately one-third of people with ASD also have IDD. Moreover, 40 percent of people with intellectual disabilities have two or more morbidities, including physical health conditions and mental health conditions, such as schizophrenia, bipolar disorder, anxiety disorders, depression, and alcohol misuse.
“Neurodevelopmental disorders profoundly impact our ability to understand what someone is communicating to us and what we’re communicating to others. Attendant co-morbidities also impact behavior and can mask an underlying neurodevelopmental disorder, delaying proper diagnosis and complicating support coordination,” explains Kathleen L. Kruse, MD, Clinical Assistant Professor at the University of Michigan Medical School’s Department of Psychiatry. “Averting one’s gaze in social communication, for example, can be characteristic of someone with ASD, and should not be considered an indicator of guilt or a sign of disrespect when being questioned by law enforcement.”
Convergence with the Sequential Intercept Model
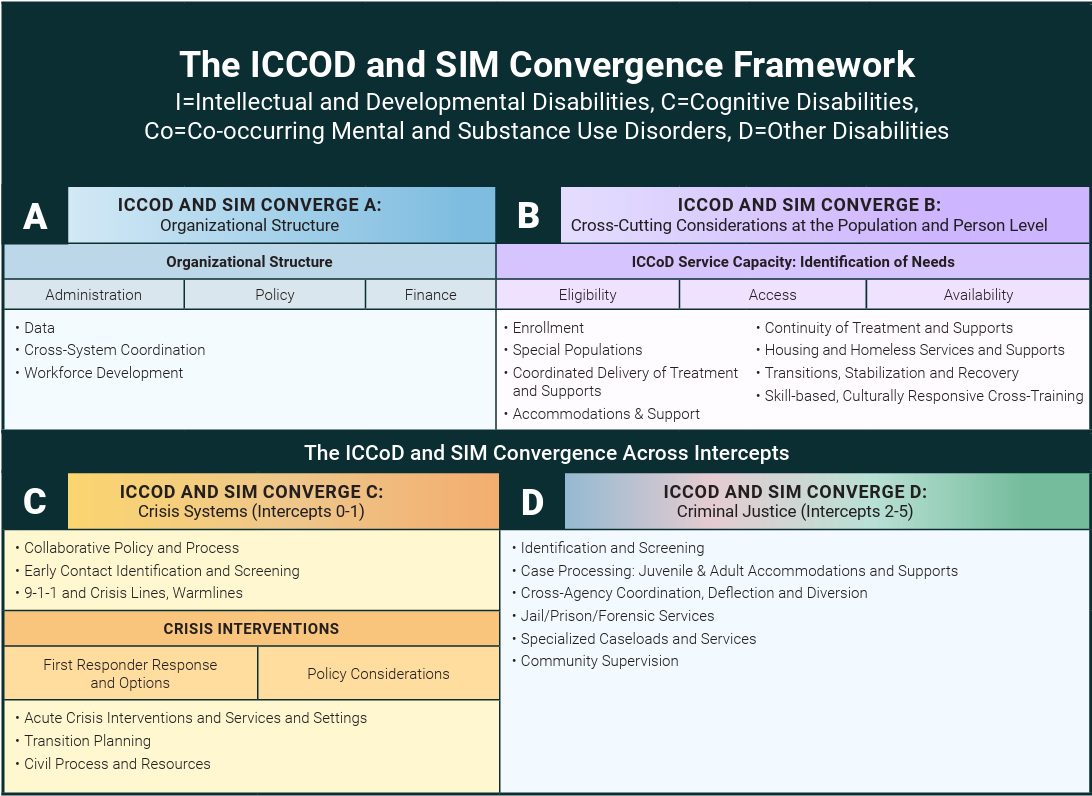
Figure 2, Developed By: Regina Huerter and Debra Pinals, 2021
Regina Huerter, Senior Project Associate at Policy Research, Inc., wholeheartedly agrees: “We must work from a universal assumption of complex needs, which demands a closer look at the Sequential Intercept Model (SIM). Support can be offered at every intercept.”
To that end, she created, with contributions from Dr. Debra Pinals, the ICCOD and SIM Convergence Framework (Figure 2). The four-quadrant framework helps individuals unfamiliar with various disabling conditions (Figure 3) understand the organizational structure (Convergence A) and service capacity (Convergence B) necessary to deliver the proper level of care. Training and funding for NDD are different than for behavioral health interventions, which can lead to limited staff confidence to properly identify, treat, and support individuals with co-occurring mental and substance use disorders.
Figure 3
Education and training are critical throughout all intercepts. Consider the trajectory of “Jesse,” a young man with ASD whose story was introduced earlier, who was questioned by a police officer. Failure to correctly interpret Jesse’s body language and non-verbal communication, combined with his eagerness to comply with an authority figure, contributed to his arrest. Notably, a desire to please is one of several adaptive behaviors associated with NDD, as is appearing to understand rights and instructions despite having difficulty doing so.
In alignment with Intercepts 0 and 1 (Community Services and Law Enforcement, respectively), Convergence C of the framework addresses the responses and options of first responders. The Crisis Response and Intervention Training (CRIT), for example, is a suggested resource for preparing police officers to respond to people experiencing crises related to behavioral health conditions and IDD.
Converge D aligns with Intercepts 2- 5 in the following ways:
Intercept 2-Initial Court Hearing and Detention: If Jesse’s competency to stand trial is questioned, a forensic evaluator trained in identifying neurodevelopment disorders will be better qualified to determine the likelihood of restoration. The Slater method is an educational program designed to help individuals with IDD achieve competency, but few facilities are adequately staffed and equipped to deliver it.
Intercept 3-Jails/Courts: Proper identification of NDD can inform eligibility for drug and mental health courts. With proper support and accommodations, Jesse may be able to participate in a specialty court that addresses comorbidities, thereby diverting him from a criminal conviction or imprisonment.
If Jesse is sentenced to jail or prison, he may have difficulty adjusting to an environment that is not only unfamiliar, but also brightly lit and noisy. He may become agitated or aggressive, not out of defiance, but due to confusion and sensory overload. Recommendations for communicating with Jesse include the following:
- Determining his primary mode of communication and using necessary accommodations.
- Speaking slowly, clearly, and calmly.
- Limiting use of facial expressions and gestures.
- Asking specific questions to prevent ambiguity.
- Avoiding frustrating questions about time, complex sequences, and reasons for behavior.
- Repeating information to improve retention.
- Allowing additional time for processing.
- Monitoring for signs of distress (repetitive speech, stereotyped behaviors, etc.).
- Cutting down on distractions.
The above tips are helpful for corrections officers, as well as for personnel providing services in Intercept 4-Reentry and Intercept 5-Community Corrections, such as staff reentry coordinators, peer support staff, behavioral health providers, social workers, and jail clinicians. Probation/parole officers are also less likely to be trained in NDD but should pay attention to how Jesse receives information and consider accommodations they can easily offer. One such accommodation could be scheduling meetings at the same time on the same day of the week at the same place out of respect for his need for consistency.
“The key to NDD is identification, so individuals can then be tested, diagnosed, and offered appropriate services,” maintains Huerter. “Ideally, this occurs during childhood, but this is not always the case for a variety of reasons, such as transience, stigma, or social drivers of health. Absent a diagnosis, we need to be able to recognize and build on functional abilities to keep individuals out of the criminal justice system and to facilitate their success.”
For More Information
- National Association for the Dually Diagnosed, an association for people with IDD and co-occurring mental health conditions.